|
|
|
| Rehabilitation Of An Edentulous Patient With Tooth Supported Overdenture – A Case Report |
Manoj Rawat 1 , Archana Nagpal 2 , Ramit Verma 3 , Jasjit Kaur 4 , Himanshu Kapoor 5
1 Private practioniser, Dept. Of Prosthodontics and Crown & Bridge - Himachal Dental College, Sundernagar
2 Professor, Department of Prosthodontics - Himachal Dental College, Sundernagar (H.P.).
3 Sr. Lecturer, Deptt Of Prosthodontics - Himachal Dental College, Sunder Nagar, Himachal Pradesh.
4 Senior Lecturer, Dept. Of Prosthodontics - Himachal Dental College, Sundernagar
5 Senior Lecturer, Dept. Of Prosthodontics - Himachal Dental College, Sundernagar
|
| Address For Correspondence |
Dr. Manoj Rawat
Rawat Niwas, Saraswati Nagar, Post Office Hartkoti
Tehsil Jubbal, Distt Shimla, Himachal Pradesh |
| Abstract |
| Overdenture has been a proven mainstay of conservative prosthodontic treatment when proper diagnosis,treatment planning, and most importantly, patient compliance are achieved. Despite recent developments indental implantology, the conservative approach to root preservation followed by an overdenture is still valid. The many advantages of root retention include- alveolar bone maintenance, better prosthesissupport, proprioceptive feedback, aesthetics and psychological benefits. This paper presents a case report ofrehabilitation of an edentulous patient with a tooth supported overdenture. |
|
| Keywords |
| Edentulous, Rehabilitation, Coping, Tooth supported overdenture |
|
| Full Text |
Introduction
Overdenture is a complete or removable partial denture that covers and rests on one or moreremaining natural teeth, the root of natural teeth, or dental implants.
Overdentures offer many advantagesover conventional complete dentures. The most important benefits are preservation of the remaining alveolar supporting bone along with increased stability and retention of the prosthesis.Retaining natural teeth under an overdenturepreserve sensory input from the periodontal receptors which are more precise than that obtained from oral mucosa. Periodontal receptors also play important role in the masticatory-salivary reflex by regulating the range and type of the masticatory stroke.
Thus, overdentures are more beneficial as they provide psychological, functional as well as biological advantages for the patients.
Case Report
This article presents two case reports inwhich overdenture applications were planned. Both the patients visited Department of Prosthodontics and Crown & Bridge, Himachal Dental College Sundernagar, Himachal Pradesh.
Case 1
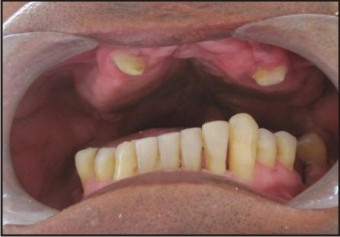
A fifty four years old male patient presented with the chief complaint of difficulty in chewing food due to missing teeth. There was no relevant medical history affectingprosthodontic treatment. Extra oral examination showed no gross abnormality. Intraoral examination revealed well formed maxillary edentulous ridge. In mandibular arch, 33,42, 43&44teeth were present. Maxillary and mandibular ridgeswerein class I ridge relationship (Fig 1). Grade three mobility was present in 42. Therefore it was advised to extract42 as a part of the treatment.
 | Fig 1 : Pre-operative Intraoral View
 |
The different treatment options available for this patient were -
1. Extraction of remaining teeth followed byconventional complete denture in both maxillary and mandibular arches.
2. Total extraction followed by implant supported overdenture in both the arches.
3. Tooth supported overdenture in mandibular arch opposing complete denture in maxillary arch.
It was decided to use the remaining teeth as abutments and fabricate an overdenture.The location of the remaining teeth wasfavourable for an overdenture. Thepatient was motivated to retain the remaining teeth in the mandibular arch.Due to economical reasons, complete denture was planned in maxillary arch.
The remaining teeth were enodontically treated. The abutment teeth were reduced in vertical height to 2mm above the crest of the ridge. The preparationwas rounded to minimize the horizontal torque on the roots. Thetooth preparation was doneto receive copings. Impression of theprepared teeth was made to obtain a cast. Wax pattern was made over the prepared teeth. Metal copings were obtained by casting and cemented over the prepared teeth (Fig. 2). Final impression, with coping in place on their respective abutment was made using a custom tray. The jaw relationwas recorded. Teeth arrangement was made and try-in was done.
 | Fig 2 : Metal Copings Cemented Over Prepared Teeth
|
Maxillary and mandibular complete dentures were fabricated following the conventional method except that the recess was created on the impression surface of the mandibular denture to accommodate the abutments (Fig. 3). The dentures were finished, polished and inserted into the patient mouth (Fig 4). The patient was given instruction about insertion and removal as well as maintenance of the dentures.(Fig 5) The post operative appearance is shown in (Fig 6). Periodic follow-up was carried out.
 | Fig 3 : Impression Surface Of The Denture
|
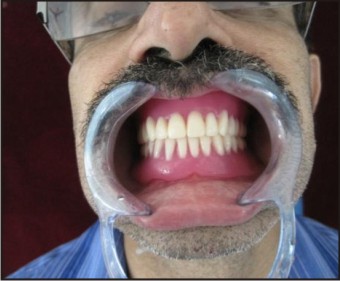 | Fig 4 : Overdenture Over Restored Abutements
|
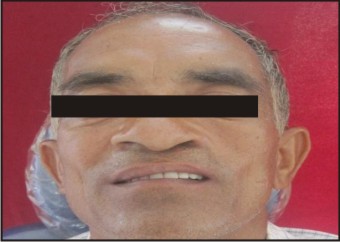
 | Fig 5 : Pre-operative
|
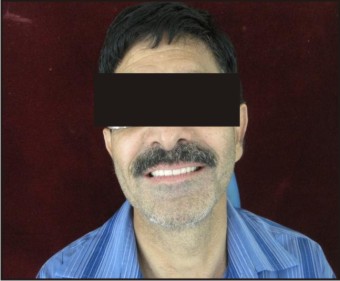 | Fig 6 : Post-operative
|
Case 2
A 46 years old male patient presented himself with the chief complaint of difficulty in chewing food. He wanted to get his missing teeth replaced.There was no relevant medical history to affect the course of prosthodontic treatment.Extra oral examination showed repaired cleft lip. Intraoral examination revealed a repaired defect in hard andsoft tissue involving the premaxilla. This defect was present due tooperatedcleft lip and palate at the age of fifteen years. In themaxillary arch13, 24 were the only remaining teeth.In the mandibular arch 31,32,33,34,35,37,41,42.43,44&45 teeth were present (Fig 1). Maxillary and mandibular ridges were in class I ridge relationship.
 | Fig 1 : Pre-operative Intraoral View
|
The different treatment options available for this patient were –
1. Extraction of remaining teeth in the maxillary arch followed by conventional complete denture in the maxillary arch and removable partial denture in mandibular arch.
2. Tooth supported overdenture in the maxillary arch and removable partial denture in the mandibular arch.
It was planned to retain the remaining teeth in the maxillary arch and use them as overdenture abutments.The location of the remaining teeth was favourable for the overdenture abutments. The patient was motivated for the treatment.
The remaining maxillary teeth were enodontically treated. Enodontically treated teeth were prepared to receive copings.Impression of the prepared teeth was made to obtain a cast. Wax pattern was made over prepared teeth. Metal copings were obtained by casting the wax pattern. Coping was finished polished and cementedover the abutments (Fig 2). Final impression was taken with copings in place on their respective abutments using a custom tray. The jaw relationswas recorded. Teeth arrangement was made and try-in was done. Complete denture was fabricated in the maxillary arch following the conventional method except that the recess were created on the impression surface of the denture to accommodate the abutments (Fig 3). The dentures were finished, polished and inserted in the patient mouth. Patient was given instruction about insertion and removal as well as maintenance of the dentures (Fig 4), (Fig 5). The post operative appearance is shown in (Fig 6). Periodic follow-up was carried out.
 | Fig 2 : Metal Copings Cemented Over Prepared Teeth
|
 | Fig 3 : Impression Surface Of The Denture
|
 | Fig 4 : Overdenture Over Restored Abutements
|
 | Fig 5 : Pre-Operative
|
 | Fig 6 : Post-Operative
|
Discussion
Fabrication of tooth supported over denture is a step in the direction of preventive prosthodontics[1]. Theresidual ridge reduction coupled with reduced dexterity at advanced age impairs the adaptation to denture prosthesis. The obvious way to prevent denture problems is to save the natural teeth.[2] Healthy teeth with compromised periodontal status can be modified and retained for biomechanical and psychological advantages. This preventive approach can be achieved by means of overdentures.[3]
Two most significant factors for the success of the overdenture are proper selection of the patient and establishing careful mode of treatment that will satisfy both the patient and the dentist.[4] Simple approach to the problem i.e. patients with congenital defects such as cleft palate, partial anodontia, microdontia, amelogensis imperfecta etc is available in the form of overdentures which will be relatively fast and inexpensive mode of treatment.[5] According to Zarb et al the advantages of overdentures include retention and stability especially the mandibular dentures[5]. The maxillary overdenture is of great value when it opposes remaining mandibular anterior teeth, because it aids in conserving the ridge against resorption from masticatory stress.[1]
Root canal therapy is a necessary phase of preparation for the selected teeth; single rooted or double rooted teeth with readily accessible canals are preferred.[6] Teeth that are mobile because of bone loss can become acceptable for overdenture support when the clinical crown is reduced to near ridge height.[6] The short coping design showed least amount of stress than any of the other design like tapered coping design& tapered coping with occlusal bearing design. This design minimizes horizontal torque on the roots[7] and provides ease of maintenance of oral hygiene.[1]
Various techniques used in the treatment of teeth to serve as abutment for overdenture ranges from simple tooth modification and reduction, tooth preparation with cast coping to endodontic therapy with amalgam plugor cast coping utilizing some form of attachments.[8] Attachments like ceka attachement and bischof-dosenbach attachement can be used but economic reasonssometime restrict their use.
The main objective in using tooth- supported overdenture is to preserve the remaining supporting tissue and to restore missing structures in such a way as to provide maximum service for maximum amount of time. A major premise of tooth supported overdenture treatment is to transfer occlusal forces along the long axis of the supporting tooth, to minimise the horizontal torque and to allow for a more optimum situation for periodontal ligaments.[7]
According to Robert L Defranco tooth supported overdenture accomplishes three important goals. It maintains the abutment as a part of the residual ridge which in turn provides more support than a conventional complete denture. When the teeth are retained, alveolar bone integrity is maintained as they support the alveolar bone. However when teeth are removed alveolar bone resorption process begins. With the preservation of the teeth there is also preservation of the periodontal membrane and this in turn preserves propioceptive impulses resulting in better occlusal awareness, biting forces and consequent neuromuscular control.[5] In routine clinical practice, overdenture should also be considered as a treatment modality for a patient who has few teeth left in the oral cavity.
Thus it can be said that the application of overdentures is unlimited and its successdepends on the dentist judgement and skill and patient motivation to maintain good oral hygiene.
Summary
Tooth supported overdentures are still an excellent and economic therapeutic concept. In this study use of root abutment as an aid to support complete denture is presented. Use of overdentures has been favoured often because of mechanical advantages. Even though the retained teeth may be periodontally compromised, they still may provide sufficient support for the transmission of masticatory pressure and periodontal ligament receptors to initiate a jaw opening reflex. The abutments enhance support and stability of the dentureand slow the rate of alveolar resorption. The clinical procedure is straightforward and can be readily applied in general dental practice.
References:
1. Wayne R. Frantz: The use of natural teeth in overlay dentures, JPD. 34: 135-140,1975.
2. Pound E. Cross-arch splinting versus premature extraction, JPD 1966; 16: 1058-68.
3. Crum RJ, Rooney GE Jr: alveolar bone loss in overdentures: a 5-year study. JPD 1978;40;610-13.
4. Toolson LB, Smith DE. A five year longitudinal study of patients treated with overdentures. JPD 1983;49;149-156.
5. Dixit S, Acharya S. Benefits of overdentures. Journal of Nepal dental association 2010;11:97-100
6. The internet journal of geriatrics and gerodontology
7. A.B Warren, A.A Caputo. Load transfer to alveolar bone as influenced by abutment design for toot-supported dentures. JPD 1975;33;137-148.
8. Henking JP. Overdentures. JPD 1982;10;217-25.
|
|
|
|
|
|
|